
Tongue Tie Infants /
Feeding Concerns

Tongue Tie in Infants
Tongue ties have associated tight muscles and joint dysfunction that affect the baby's ability to suck, swallow or breath, in some feeding positions. For example, if the temporal mandibular joint of the jaw (TMJ) is restricted, the baby cannot open wide. This can lead to a shallow latch, or the baby slipping off the breast or compression of the nipple.
If muscles of the jaw, mouth, or tongue are tight, their function is weak. Weak muscles have less endurance. Babies will get tired and sleepy at the breast as they get tired from working too hard to drink milk.
Tongue-tie (ankyloglossia) is a problem that is present at birth. It happens when the tissue that attaches the tongue to the bottom of the mouth (lingual frenulum) is too short. This can limit the movement of the tongue.
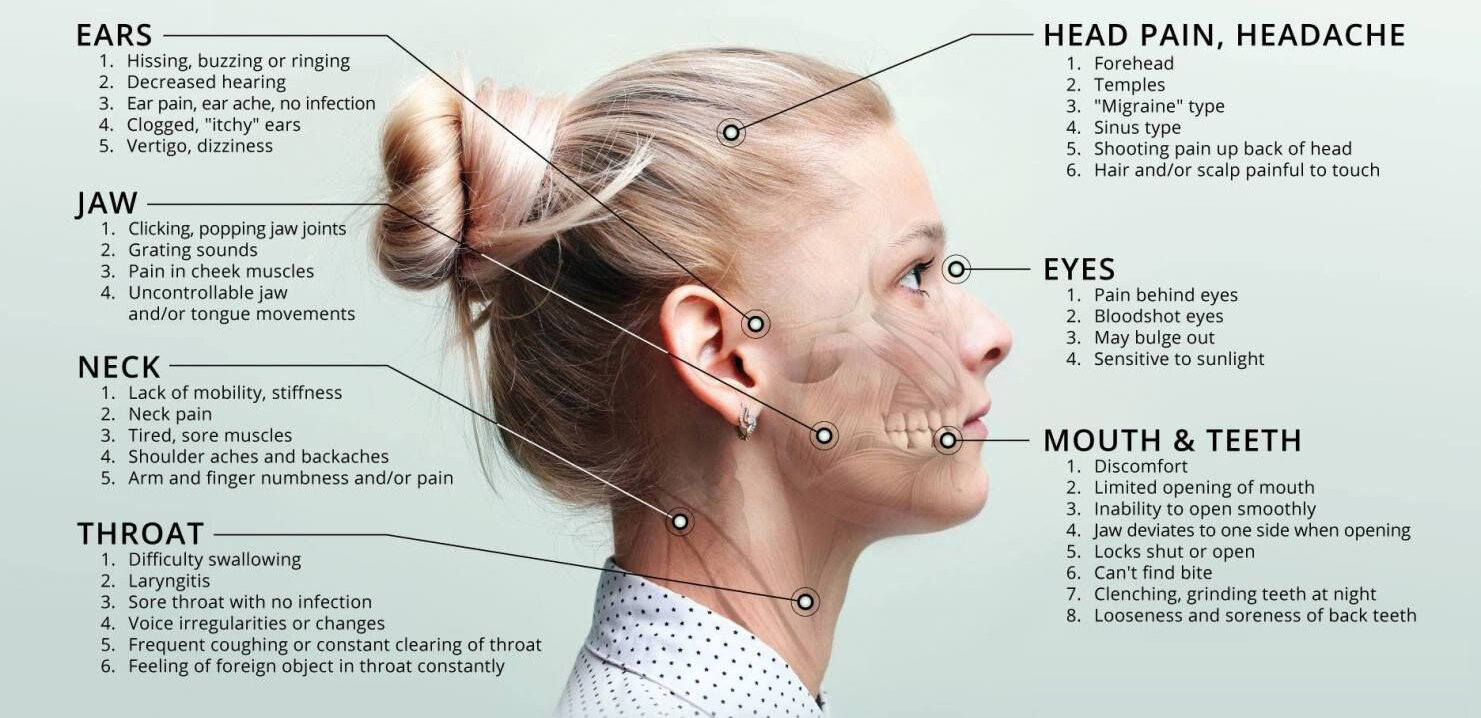
The restriction caused by a tongue-tie can lead to changes in the development of the mouth, face, and skull, and are often accompanied with an open mouth posture or mouth breathing in children. This can in turn lead to symptoms including speech difficulties, ADD and ADHD, sleep disordered breathing and conditions such as sleep apnea, and jaw and facial pain/tension.
What are some signs and symptoms of a tongue restriction?
Shallow latch
Chugging while feeding
Short time between feeds
Clicking while feeding
Difficulty latching on or sucking from the breast
Mother in significant pain while nursing
A baby who constantly fusses at the breast
Milk leaking out of the sides of the mouth
Poor milk transfer, poor weight gain and failure to thrive in an infant
V-shaped or heart-shaped notch at the tip of the tongue when it’s stuck out
A toddler’s difficulty in licking a lollipop or ice cream cone, touching the roof of their mouth, moving their tongue from side to side, or sticking out their tongue past the upper gums
Enunciation problems that continue after age 3, especially when articulating these sounds: t, d, l, r, n, th, s, and z
Persistent dental problems, such as a gap between the front lower teeth and tooth decay or gingivitis (gum inflammation) because your child can’t get rid of food debris naturally with her tongue
Difficulty chewing age-appropriate solid foods
Gagging or choking on foods
Persistent dribbling/drooling
What is a Frenectomy?
A frenectomy, also referred to as frenulectomy, frenuloplasty or functional frenuloplasty is a simple incision into the connective tissue at the bottom of the tongue to free the tongue from the floor of the mouth. This involves removing or altering the connective tethered tissue under the tongue. In the majority of cases, the procedure is done using local anesthetic as general anesthetic is rare with this procedure. The procedure is low risk and can be performed with a laser, a scalpel, or scissors. When it’s done by laser, no sutures are required. With a scalpel or scissors, sutures will be placed to help the wound heal. Wound healing usually takes one to two weeks, although it may take longer.

Has your baby had a tongue tie release surgery that was unsuccessful?
We see this quite often with babies/toddlers that get tongue tie releases at an early age without preparation and optimal timing. The orofacial muscles and connective tissues require therapeutic measures to reduce compensations and optimize functional movement. This can be assessed and addressed up until the age of 12 months. An examination by a Myofunctional Therapist can take place once again at the age of 3-4 years old. If the tongue has some re-attachment and still presents with a restriction, myofunctional therapy can be introduced with the possibility of a frenectomy revision.
Pre and post operative myofunctional therapy is essential for optimal recovery and to achieve the desired results.
-
Myofunctional Therapy Wellness Program
Improved sleep & Increased focus and concentration at school
Kelly is amazing to work with! She did such a good job explaining the process and what we should expect. She made our shy child feel safe and he gained confidence working with her through the program.
James was quick to heal after the procedure and we have seen significant improvement in his breathing, restful sleep, and flexibility (this one surprised me).
The improve sleep quality seems to be having a positive impact on his attention to school work and his overall demeanour.
We would certainly recommend working with Kelly!
On behalf of:
~James, W.,age 12
-
Mini Myo Program - Ages 4-6 years
Speech clarity & Healthier breathing
My 4 year old daughter was recommended by her dental hygienist to go see Kelly due to what they thought could be a suspected lip tie, which they thought could possibly cause issues with her teeth later on. We went and had a thorough assessment and ended up deciding to do the Mini-Myo program.
Over the course of the program, we noticed visible changes in our daughter’s oral habits. Her oral muscles have gotten much stronger, and we have learned how to encourage proper tongue placement, something we continue to practice and have noticed a difference in her overall breathing and even some clarity to her speaking.
With the knowledge and exercises Kelly taught us, we have begun the process of teaching our other, 7 year old daughter the exercises we’ve learned throughout the program. Kelly helped me set up a program that I could continue myself for her and gave us some advice and guidance on what we should be advocating for in the future, in terms of orthodontic treatment.
The exercises are so fun and tailored to the child’s age. Both my kids look forward to doing them every night, we even have our 2 year old join in with some of the easier ones as well.
We are so thankful to Kelly for all she’s taught us and plan to recommend her to anyone who needs this type of therapy!
On behalf of
~Marquesa, C, age 4
-
Enhanced Myofunctional Therapy Program
TMJ pain & TMD
I was referred to Kelly by my orthodontist to address my open bite and tongue thrusting. I had also been experiencing chronic TMJ pain. I immediately established a great connection with Kelly and looked forward to what she had in store for me.
She expressed right from the beginning how important it was to stay consistent with the exercises that she provided…. I took her advice and practiced my exercises daily…. The main focus was me and my comfort levels.
She encouraged me to push myself each time but never to exceed my limits. Kelly also taught me about bad oral habits and how it can affect other areas of the body. I was able to learn about my own oral habits and how to properly correct them to achieve my goals. With her expertise, Kelly was also able to identify that I had posterior tongue tie and very restrictive frenums (the web-like attachments inside the lips and cheeks).
As per her recommendation, I had these issues addressed by a specialist. After going through with the procedures, I had incredible relief from the release of my tongue tie and restrictive frenums.
I made outstanding progress by following the plan Kelly had created just for me. I no longer have an open bite, my tongue thrust is under control, and my jaw pain has disappeared.
I would highly recommend her to anyone who’s in need of an OMT.
~ Kayla, F.,age 29
-
Mini Myo Program - Ages 4-6 years
Delayed speech & Tongue posture
It was recommended to me by a Speech Pathologist that I take my daughter to see a Myofunctional Therapist when she was about 4.5-5 years old. At the time of the recommendation, she was 3 years old, displayed speech issues and hearing loss from water in her ears. Tubes placed in her ears totally corrected her hearing, but her speech was still affected.
I chose Back to your Roots OMT as I felt after doing an Myofunctional Therapy assessment with Kelly, that she truly was an expert in her field and Shylah really enjoyed to be around her.
Kelly was able to identify what Shylah's specific orofacial concerns were with her tongue placement, resting posture and speech; problems that had not been addressed in the past that were quite critical to Shylah's speech and oral development. Shylah did not have proper resting tongue posture that was affecting her speech and the proper growth and development of her jaw.
Shylah also was in need of a frenectomy, as she presented with an upper lip restriction. These issues were addressed and corrected with Kelly's guidance and therapy for Shylah.
I was also very curious on how exactly Kelly was going to manage keeping my very busy and vivacious junior kindergartener focused on mouth activities that would need to be done daily. Kelly makes therapy super fun!! Shylah was so excited for her meetings with Kelly and to practice her exercises that to her were just games. Kelly had shown us how to incorporate these exercises into our lives in a truly organic way, so it wasn't anything stressful or felt like a chore for Shylah. Shylah loved them!! They were really fun games for her.
We almost immediately saw improvement in Shylah's speech, tongue and overall mouth strength. By the end of the OMT program Shylah had many tools to work with to keep her mouth, lips and tongue functioning in tip top shape.
We are so grateful for Kelly and her expertise. She has really helped Shylah to overcome all the challenges she was having with her orofacial muscles.
On behalf of:
~Shylah, W., age 4
-
Myofunctional Therapy Wellness Program
Tongue thrust & Tongue tie
“It was such a great experience to work with Kelly these past few months. I was unsure at first about myofunctional therapy, but I really wish I had known about it sooner.
I had braces about 12 years ago and only found out about my tongue thrusting habits and tongue tie this year as I noticed a significant change in my bite. Fortunately,
I was referred to this program with Kelly and I am happy to say it was a great success! Not only do I feel better, but I am also more aware of my habits and have seen great improvements with my tongue posture, breathing, sleep, and overall health.
I would highly recommend working with Kelly. She was very well organized, informative, and encouraging throughout the entire program.”
~ Angel, O.,age 24
-
Enhanced Myofunctional Therapy Program
Orthodontic relapse & Open bite
“When my orthodontist referred me to Kelly Hall, I was estimated to need braces for 18 months to fix my open bite and I had jaw pain that was a 7 on a scale of 1 to 10. After three months of working with Kelly while wearing braces, my open bite had almost completely closed, and after six months it was completely closed! I cannot be more thrilled about how quickly my bite changed and I am happy that Kelly has provided me with the knowledge and tools to keep my bite closed after my braces come off. In addition to the dental benefits, I have also noticed improved sleep, stress management, and digestion through taking Kelly’s program. It is crazy how much of a difference that proper breathing, chewing and swallowing makes!”
~ Christine, H., age 25
-
Mini Myo Program - Ages 4-6 years
Tongue posture & Facial growth
My family and I could not be more thrilled to have had the opportunity to work with Kelly. We approached Kelly to assist with our 5 year old’s tongue posture. Kelly listened to our initial concerns, and set up a very detailed program plan for our son. The entire program was fun, yet challenging enough to keep our son engaged. Kelly was always willing to go above and beyond to help answer any questions we had throughout the program. Not only have we noticed a dramatic difference in our son’s tongue posture and facial shape, Kelly’s before and after pictures confirmed our progress. Thank you, Kelly!
-
Myofunctional Therapy Wellness Program
Less headaches/jaw pain and Improved sleep
I absolutely LOVED working with Kelly! I never knew I was struggling with so many issues as a result of poor tongue posture, but by the end of the program, I have noticed such a huge improvement. I am doing orthodontics for the second time and learned that my teeth had shifted from incorrect tongue posture. Working together over a span of 6 months helped create healthy habits that I will continue to build on a daily basis. I am so aware of where my tongue now belongs, and I no longer mouth breathe as my first instinct. I don't snore as often, and as a result, I get a better sleep through the night, have less headaches overall, less jaw pain, and even better digestion/less bloating. I now have access to the tools and habits to continue to improve my symptoms even after we finished working together. I felt completely supported and feel confident that I can take what I have learned and continue to build those healthy habits. So glad I took the leap! :)
~Tia, A., age 26
-
Enhanced Myofunctional Therapy Program
No more Snoring & Jaw stability
I am a 68 year old woman who recently completed a OMT Enhanced Program with Kelly Hall. I am thrilled at the results and with my experience. Having a Frenectomy, coupled with the OMT exercises, released the muscle tension in my mouth, face and jaw. No more hyper mobility in my jaw or TMJ pain; I finally have a symmetrical mouth; my tongue is supporting my upper jaw (who knew it was supposed to do this); my snoring has all but disappeared; and my swallowing has greatly improved. I didn’t realize these problems, built up over years of being tongue tied, could be remedied, let alone to the extent they have. I highly recommend this treatment for anyone who has a tongue tie--the younger the better. I also highly recommend Kelly Hall. She is very knowledgeable about the treatment regime and extremely supportive of her clients.
~ Sharon, F., age 68
-
Mini Myo Program - Ages 4-6 years
Facial growth & development
“Kelly was great at taking us through the Mini Myo program for our kindergartener, and we started seeing improvements in just a few months. We have a long road ahead of us to correct mouth breathing habits and widen palate, but we now have a great foundation of exercises and practices tailored to our child's needs that we can continue with to improve breathing and overall health. Thanks Kelly!”
On behalf of:
~Alexander, N., age 5
-
Myofunctional Therapy with a Frenectomy
Tongue tie Release: Postural Improvements
“I wasn’t sure how a tongue release would impact my treatment but, since having the frenectomy procedure, I wish that I had it done sooner! I have already noticed significant changes in my posture since having my tongue tie release and I am looking forward to observing the benefits of the release throughout my future appointments with Kelly Hall.”
~ Christine, H., age 25
-
Kind words from parents
#1 Thanks for your patience today - a tired kid after late nights on the long weekend combined with eating barely any of his lunch and that’s what you get! Appreciate your patience and kindness!
#2 Thank you so much for calling me today. You really do go above and beyond for helping us to adhere to the therapy sessions and you do a great job dealing with my super emotional children.
-
Mini Myo Program - Ages 4-6 years
Mouth breathing & Tongue thrust
“We were so lucky to find Kelly as I can attest that the program works and helped my son the way he needed. it was night and day. By following the exercises we were able to correct his tongue thrust, and soon the benefits of nose breathing started to payoff, he was sleeping better (continuous deep sleep) and no more headaches. Without hesitation I would recommend Kelly and this therapy for young kids, specially as the the program is designed to be fun and got my kid engaged on the exercises since the first session.”
On behalf of:
~Omar, R., age 6
-
Myofunctional Therapy with a Frenectomy
Tongue & Lip Tie Release: Instant relief of neck & shoulder tension
"It has been a joy to work with Kelly over the duration of this program! I wasn’t sure if anything could help my tension, headaches, jaw pain, and breathing issues, but now I truly wish I had found Kelly sooner. After having my lip and tongue ties released, I felt instant relief. I couldn't imagine doing the procedure without Kelly's support. Combined with the exercises in the program, I’ve noticed that it is easier to breathe, I have had a decrease in neck and shoulder tension, and have improved my posture and flexibility. I am looking forward to having my daughter go through the children’s program and am relieved that she will not have to deal with the same pain that I did before I found help.”
~Hunter, C., age 26
-
Kinds words following an OMT Evaluation
I am finding that the CPAP is really comfortable (now that I found the right mask) and I have fully adjusted to it. Thank you for encouraging me to be compliant with it - it was a life changer!
Your advice greatly changed my quality of life so THANK YOU!
-
Myofunctional Therapy Wellness Program
TMD / Jaw Pain
Kelly has been instrumental in helping my daughter go from extremely painful TMJ symptoms and on medication to having little to no pain and off all meds. Her patience and understanding made my daughter feel comfortable and willing to open up to her. I would highly recommend Kelly "Back to your Roots Orofacial Myofunctional Therapy".
On behalf of:
~Sarah H., age 20
-
Mini Myo Program - Ages 4 - 6 years
Better Sleep & Improved Digestion PLUS a Growth Spurt
As a Mom of 4 boys (9yrs & under) and having worked as a Hygienist myself for over a decade, I wanted to seek out an OMT that was not only immensely knowledgeable, but also someone who could make the therapy appointments work with our VERY busy schedule! Kelly provided all of this and more!! From the initial assessment, her knowledge & passion was up front and center, and throughout the therapy appointments she even taught me quite a few things!
It was our 6yr old son going through Kelly’s ‘Mini Myo’ program and it was SO perfect for a child. She started off with very easy and fun exercises to gain his interest, and slowly built up as his abilities progressed. As many 6yr olds, he can get a little restless and uninterested as weeks passed on, but Kelly was right on the ball and had many suggestions to make it all “new” and “exciting” again!
The virtual appointments were extremely thorough and made it very easy for our very hectic schedule. Video quality was excellent and myself & my son could see exactly what Kelly was demonstrating clearly.
When it’s time for our next child to go through the program (many of the concern’s OMT therapies treat can often be seen in other family members, which is the case for our family) I won’t hesitate to contact Kelly!
Thank you so much, Kelly! You made it all so easy and the changes we have seen in our little guy (sleep apnea’s gone, mouth breathing is gone, stomach ‘gassiness’ gone, greatly improved sleep quality, as well as a growth spurt! The list almost feels endless!) made the investment in time and cost SO worth it!!
On behalf of :
~Parker, G., age 6
-
Myofunctional Therapy Wellness Program
Tongue tie release / No more clenching
I was referred to Kelly by the dentist who assessed my tongue tie. At the very first meeting, she was very welcoming, knowledgeable and I signed up for the therapy course right on the spot knowing it was the right decision. She right away explained my very restricted tongue tie and its effects for over 30 years was an eye opener. Sessions with Kelly were great, learning new exercises in order to build up to the release and after. They were very structured building upon each one to strengthen and train the tongue.
After the release I immediately felt tension released in my shoulders and neck, flexibility improved and I now do not clench my teeth during the night. Kelly helped make this experience very smooth and successful! I recommend anyone who may have some questions or concerns about tongue tie to see Kelly!
~John, Z., age 34
-
Myofunctional Therapy Wellness program
Jaw stability & Resting tongue posture
A wonderful practitioner to start your myo journey with she will provide you all the tools and knowledge you need to achieve your goals. She's lovely please do see her!
As a young adult who took her own oral postural health as a priority after experiencing adverse symptoms and learning more about the ill effects , I've only wished I started sooner. Highly recommend this therapy and Kelly I've achieved results that exceeded what I thought I could achieve !
~Anastasis, Oh., age 22
-
Enhanced Myofunctional Therapy Program
Tongue Tie release & Decreased tension
I am in my late 50's and when my (young) dental hygienist informed me that the inside of my mouth was smaller than most and I was a bit tongue tied, I didn't care... been that way all my life and its never come up as an issue so why does it matter? But she noted that her and I have similar physical symptoms; crushing insomnia, daily headaches, teeth grinding, lots of neck & shoulder tension and soreness around the TMJ area to name some. She told me how she found relief through an OMT therapist (Kelly Hall in Cambridge, who is excellent by the way) and was so impressed that she is formally studying OMT and intends to specialize in it.
Of course, my dentist backed her up and referred me to Kelly - did I mention that Kelly is awesome!?!
I am always skeptical of claims like these - the ones that sound too good to be true - but I did some research on my own before committing to it and decided to go for it just in case I could find some relief myself. And I'm so glad I did. About 2 months into my treatment package, Kelly referred me for a frenectomy. Before my procedure she videoed some range of motion tests she had me perform. To my surprise & relief, the procedure itself was MUCH less painful and unpleasant than getting a cavity filled - my god... that needle is the worst! After all the medical advancements they still use that massive archaic freezing needle for cavities. The needle for this procedure is much smaller and thinner. They applied a topical numbing agent first and I barely felt the needle under my tongue. The freezing I got under my upper lip hurt a bit more but still very tolerable. After that, I felt nothing.
A CO2 laser was used so there very little bleeding and trauma. Near the end of the procedure, she asked me to perform those range of motion tests again and no word of a lie, I easily went further on all 4 of them. Then she says, 'wait a minute' and she made another cut or two and asked me to turn my head to the right side again and I went even further! I was really impressed how a few snips inside my mouth allowed for more movement in other parts of my body. The last thing she asked me was what number my pain was at now (I was an 8 before we started). Because I was so focused on what was happening in my mouth, I had to tune back into it and had a hard time finding it.
This was the most astonishing thing to me. The tension in my shoulders, neck, jaw and head was pretty much gone!! I was now at a 3. For the last 10 years at least, my normal daily pain set-point has been between 5 and 7 so to get instantly to a 3 was unimaginable to me. The tension was just gone... lifted... disappeared. So I continue my bi-weekly sessions with Kelly but I'm no longer skeptical. I look forward to getting the next set of exercises which I expect will help me improve some of my other areas of malfunction.
~Michelle, P., age 57
-
Myofunctional Therapy Wellness Program
Orthodontic retention & Resting tongue posture
I was referred to Kelly through my orthodontist. i started my sessions with her because i had a bad tongue placement. I was skeptic walking into the program because i didn’t know how effective it would be getting this treatment at 23 but i kept an open mind. After a long questionnaire and consultation i actually realized how bad my tongue placement was, and how it was affecting my lifestyle activities, such as my eating , sleep, breathing and so on.
The activities were very interesting and some challenging, but I can confidently say that my tongue sits in the perfect position now, and I am truly amazed about how far I have come. My sleep is so good now, my eating is perfect and so is my breathing. This also benefits my ortho treatment because my tongue will not affect my jaw anymore.
I highly would recommend this treatment to anyone and Kelly is amazing because you never know that you actually do need Myo.
~Ibifuro, D., age 23
-
Mini Myo Program - Ages 4-6 years
Jaw growth & Improved regulation of behaviour
My five year old and I had a great time working with Kelly for the Mini-Myo program. Before starting we were dealing with mouth breathing, poor sleep and some behavioural issues (a lip tie, tooth decay, a cross bite and very small and narrow jaw, too). We wanted to address the root cause of these symptoms and ended up connecting with Kelly at Back To Your Roots OMT. She always made our sessions fun and engaging and offered adaptive alternatives when needed.
By our final session my daughter started breathing, sleeping and eating better and many of her behavioural issues have since resolved. In addition to this, we noticed a significant change in her height and facial growth in a short period of time.
We are excited to continue with what we have learned from Kelly and continue to see more improvements in the months to come.
On behalf of:
~Zaynab, M., age 5
-
Myofunctional Therapy Wellness Program
Improved posture & Improved swallowing
Can't say enough about how amazing the experience was with Kelly.
I dealt with insecurities surrounding my posture, swallowing and nasal breathing for years. I felt comfortable sharing my experiences and goals in a collaborative and supportive setting in our sessions. Kelly gave me the confidence to ensure I was on the right track, now, and into the future.
It was a difficult decision to commit time and energy as an adult to a myofacial practice, but the rewards have been well earned. I'm forever grateful for what I've learned and knowing that Kelly is a resource, now, and in the future.
For anyone else struggling out there as an adult with post-traumatic ortho. Consider myo as a place to rekindle your confidence with nasal breathing, proper chewing and swallowing and a guide to better health.
~Adam, T., age 39
-
Enhanced Myofunctional Therapy Program
No more jaw pain & Physical changes
My entire experience with Back to Your Roots was incredible from start to finish! In 6 months my constant jaw pain and discomfort had disappeared completely and I have noticed physical changes to my appearance as well. You do need to hold yourself accountable and put in the work but Kelly makes your exercise routines easy to work into your daily life.
Thank you Kelly!!
~Courtney, T., age 35
-
Mini Myo Program - Ages 4 - 6 years
Speech clarity & Improved sleep
Our experience with Back to Your Roots OMT and Kelly has been nothing short of amazing. From the moment we connected, Kelly went above and beyond our expectations. We started OMT just before our son turned 4, he had been showing signs of a tongue tie, but no one seemed to agree. Kelly, however, instantly confirmed what we had suspected and seamlessly connected us with an excellent dentist for the necessary release.
We have witnessed remarkable improvements in his mouth posture, tongue range of motion, tone, and speech sounds. We are immensely grateful for Kelly's expertise, dedication, and her ability to engage our 4 year old. We wholeheartedly recommend her services to anyone in need and look forward to continuing our journey with Kelly.
On behalf of:
~Henry, M., age 4
-
Myofunctional Therapy Wellness Program
Jaw comfort & tongue posture
My experience working with Kelly was excellent.
Appointments were easily accessible online and our time spent together was always organized and thorough. My jaw tension improved as I learned to correct my resting tongue posture through the guided exercises Kelly taught me. I can tell my orofacial muscle coordination and strength has improved over our time working together.
I would (and do!) highly recommend Kelly and her OMT program to everyone with TMJ dysfunction, jaw pain, and tension headaches.
~Victoria, H., age 31
-
Myofunctional Therapy Wellness Program
Tongue tie & Deeper Restorative Sleep
I went to see Kelly to fix my tongue tie. After finishing the therapy, not only is the tongue tie fixed, but I sleep better, speak more clearly, eat properly, and have more energy.
She was knowledgeable, accommodating, and happy to answer any and all questions. I wasn't expecting the noticeable improvement I saw in everyday life, and I'm very happy with the results.
It was a great experience from start to end, and I would absolutely recommend it.
~Kurt, E., age 31
-
Enhanced Myofunctional Therapy Program
Tongue posture & Oral muscle balance
Kelly is a patient, caring, very skilled, and thorough practitioner. She identified and adapted to my learning style very quickly, and I had great results.
I appreciated her advocating for the most minimally invasive approach to dealing with my presenting issues, and I managed to avoid painful surgery while greatly improving my oral functioning, which was an ideal outcome!
I am very fortunate to have worked with Kelly, and I recommend her services without reservation.
~Jean, G., age 33
-
Myofunctional Therapy Wellness Program
Whole body approach / Health & wellness
My son was initially seeing an OMT closer to home but we weren’t happy with the service so we searched for another provider hoping to find someone locally but stumbled upon Kelly’s website.
Her whole-body approach to Health & Wellness resonated with me and right from our first contact with Kelly, she was professional and friendly. She explained everything thoroughly and we knew exactly what we were supposed to do and why (which wasn’t the case in the past). She is very organized and her communication skills are exceptional.
We are from BC and were worried about having an OMT we couldn't see in person but this wasn’t an issue at all. While we are sad that the program is over, it also means that she accomplished her goals of helping our son and we are forever grateful for her compassion and ability to connect with him.
Both myself and my son wouldn’t hesitate to recommend Kelly to others.
On behalf of:
~Luke, S., age 10
-
Myofunctional Therapy Wellness Program
Facial symmetry & improved cognitive function
I am so grateful to have found Kelly at Back to Your Roots Orofacial Myofunctional Therapy.
This therapy has been extremely beneficial to my daughter in helping her to regain symmetry in her face after an injury to her cheek.
As well, the unexpected benefits of better sleep, posture, and breathing habits have made a huge difference to her daily life.
On behalf of:
~Kaiya, S., age 14
-
Enhanced Myofunctional Therapy Program
Mouth breathing & Headaches
I am so thankful to have had the opportunity to work with Kelly Hall. From our initial appointment all the way through to our final appointment Kelly has been knowledgeable and dedicated to my care.
While working with Kelly over the past 6 months I was able to get rid of headaches that were caused by TMJ. The exercises and tools she gave me are easily worked into my daily routine and will ensure the pain stays away even though we have finished the program.Mouth breathing was my main concern when I first started meeting with Kelly. She taught me alot about form, and the proper mechanics for becoming a nose breather, which is something I didn't think was possible. I am now able to breathe through my nose and am working on transitioning to breathing through my nose all of the time.
I would recommend Kelly to anyone who is looking for myotherapy services. She provided a supportive environment that encouraged both healing and learning.
~Liz, M.,age 33 -
Mini Myo Program - Ages 4-6 years
Growing a healthy jaw
I have brought my 6 year old son to Kelly for preventative reasons.
Main concern was crowding of teeth. It is still too early to see changes (only have been doing exercises for about 5 months now). However, I remain hopeful that the significant improvement seen so far in his tongue posture up against his palate will help push on the bone structure and widen his palate as he continues to grow - allowing more space for his teeth!
Kelly has been absolutely amazing with my son. Playful when appropriate and serious to get him back on track when needed. A great manor with children.
I highly recommend Kelly.On behalf of:
~Mack, D., age 6